Pre-authorizations
Request, submit, and record payer decisions with a full lifecycle — and the split engine enforces approval before covered service where the payer requires it.
One core, shared services, ten modules — the two-minute architecture tour.
Explore the platform →Ten modules on one patient record and one ledger — no seams, no re-entry.
See the products →Be first — on terms that make first safe. Staged payments, escrow, founding pricing.
Explore the programme →Score your facility across ten dimensions in fifteen minutes.
Get the workbooksoonProduct — Revenue Cycle & NHIS
Charges post the moment care happens. The payer's share and the patient's share split themselves. And the monthly NHIS claim — ICD codes mapped to G-DRG, per-encounter CCC, validated against payer rules — generates in seconds instead of days. Cash, NHIS, private and corporate payers, on one engine.
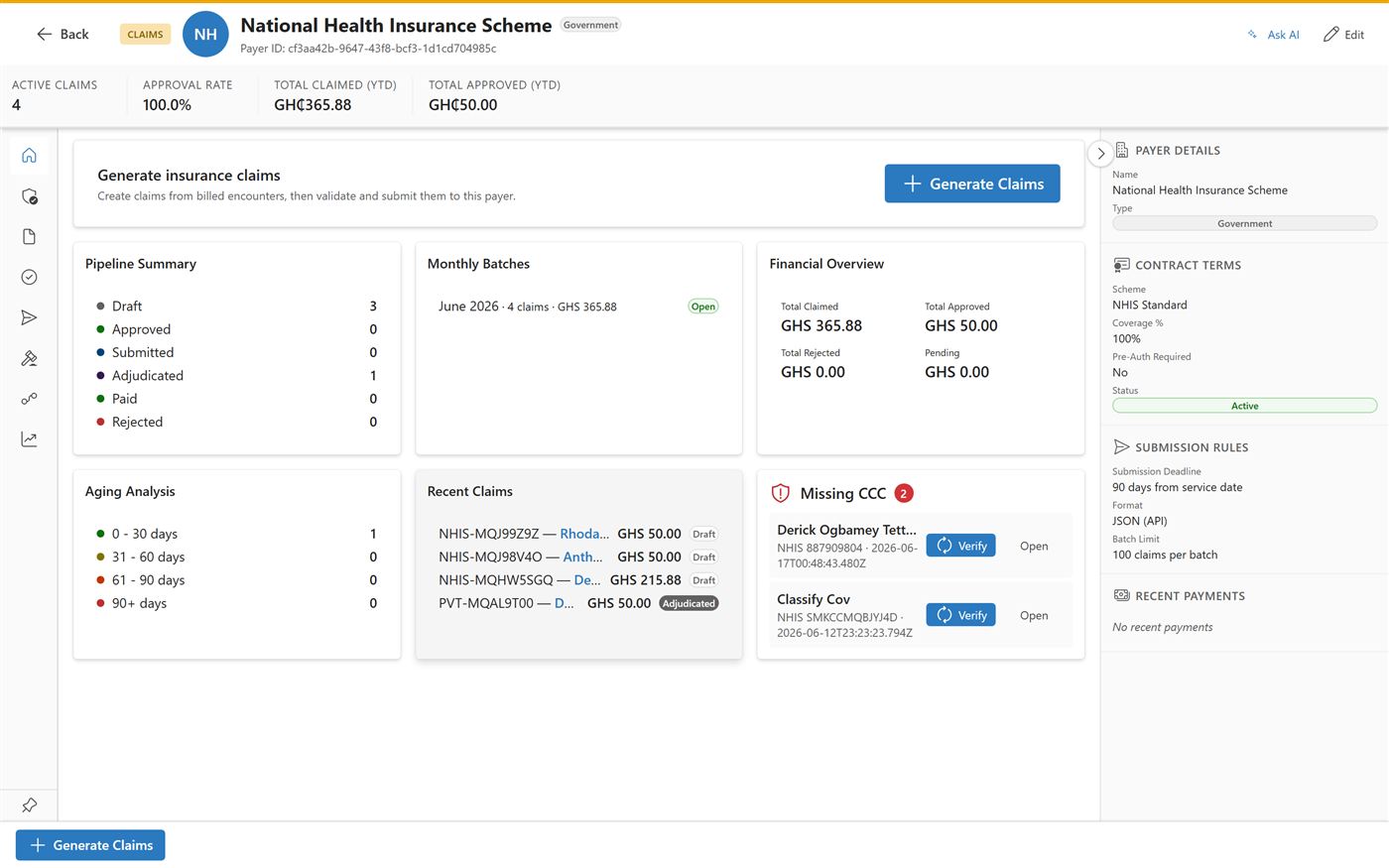
Live product — NHIS claims workstation, test data.
The problem
In hospitals running disconnected systems, services delivered in one department routinely never land on the bill. DDRT is designed to capture the charge at the point of care — a capability, not a promised percentage.
Paper NHIS claims are rejected around ten percent of the time, versus one to three percent submitted electronically. Clean, validated files get paid.
Nonvignon et al., 2022A manual monthly NHIS file costs a claims officer days of transcription — and every transcription is a chance to be rejected. DDRT generates the file from data that already exists.
How it works
Five stages, no re-entry anywhere. Each stage feeds the next from the same record.
A consultation, a lab order, a dispense, a bed-night — every billable clinical action creates its charge at the moment it happens, priced from your tariff for that payer. No end-of-visit reconstruction, no forgotten services.
The engine knows the patient's coverage — NHIS, private insurer, corporate scheme, or cash — and splits every line accordingly: what the payer owes, what the patient owes, collected as configured. Pay-as-you-go gating and deposits are supported where your policy requires them. NHIS membership is verified at registration, and the encounter's claim check code (CCC) is captured at the point of service — not hunted down at month-end.
Diagnoses map automatically from ICD codes to G-DRG bundles, medicines and consumables price from the NHIS medicines tariff, each encounter carries its captured CCC, and batches export in NHIA's format (XML v8.6). What took a claims officer days now takes the time it takes to click Generate.
Every claim is vetted internally against NHIA rules before submission — missing CCCs, coverage mismatches, and out-of-window encounters are flagged with one-click fixes. The 90-day deadline is tracked per claim, and a rejection dashboard turns every vetting deduction into a rule for next month.
Cash, mobile money, and card payments reconcile per cashier shift. And because DDRT includes a real general ledger, every payment, claim, and adjustment posts its journal entry automatically. Month-end is a review, not an archaeology dig. And when the NHIA remittance arrives, it reconciles claim by claim — paid, adjusted, or rejected — so vetting deductions are visible and disputable, never silently absorbed.
One screen for the claims office
Totals claimed and approved, per-payer workstations, aging since submission, and an attention queue that stays empty when you're on top of it.
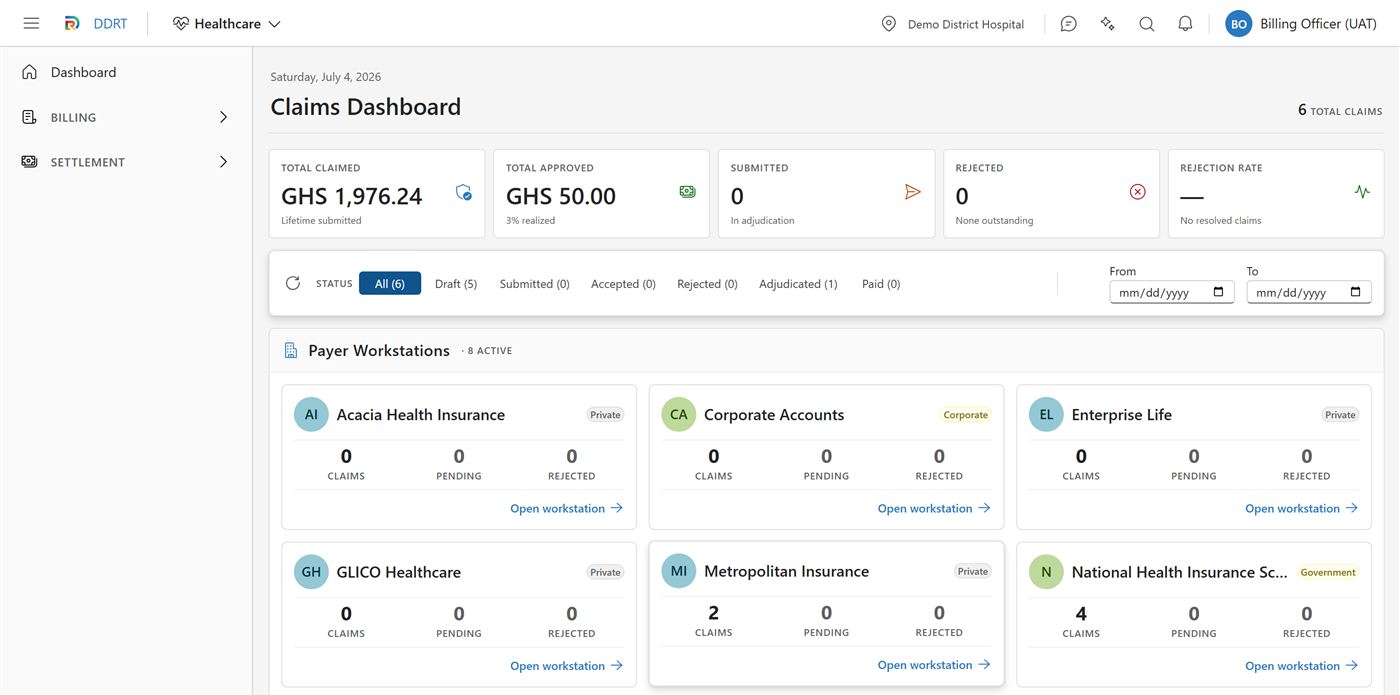
Live product — claims dashboard, test data.
Also in the box
Request, submit, and record payer decisions with a full lifecycle — and the split engine enforces approval before covered service where the payer requires it.
Price schedules per payer and facility, G-DRG tariff import for NHIS, and a price tester to verify what any service costs any patient before it's charged.
MoMo and card tenders alongside cash, with per-shift reconciliation that separates cash-drawer expectations from PSP settlements and fees.
Configurable gating for services that require payment or deposit first — enforced by the platform, with clinical-safety overrides where policy demands them.
NHIS is the headline, not the limit: private insurers and corporate schemes run the same claim lifecycle with their own rules, formats, and statements.
Refunds and billing adjustments run approval workflows with separation of duties — and land in the audit trail and the ledger like everything else.
Why it works
Standalone billing systems leak because they only know what someone remembers to type into them. DDRT's revenue cycle sits on the same record as the clinic, the lab, and the pharmacy — the charge exists because the care exists. That's the platform argument, and it has its own page.
Next step
In the demo, we'll walk a patient from registration to a validated NHIS claim in one sitting — then compare it with how last month actually went.